Epididymitis is an inflammation of the epididymis, a coiled tube located at the back of the testicle that is crucial for the storage and maturation of sperm. Varicocele, on the other hand, is a condition characterized by the abnormal enlargement of the veins within the scrotum. The potential causal relationship between epididymitis and varicocele is an area of interest in the field of urology and male reproductive health. Understanding this relationship requires a detailed exploration of the anatomy, pathophysiology of both conditions, and the possible mechanisms through which one might lead to the other.
Anatomy of the Epididymis and Testicular Vasculature
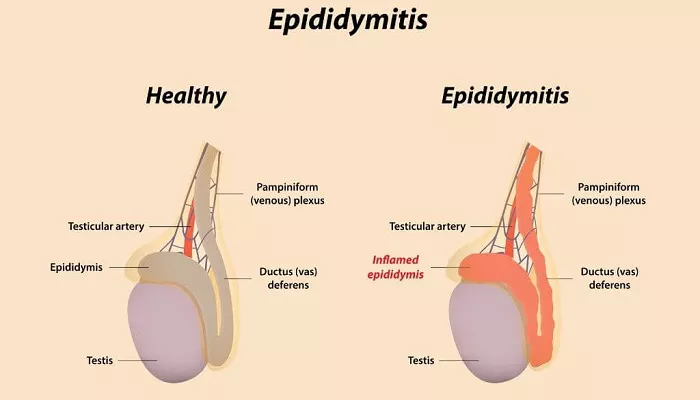
The epididymis is closely associated with the testicle and is supplied by a network of blood vessels. The testicular arteries bring oxygenated blood to the testicles and epididymis, while the pampiniform plexus, a group of veins, is responsible for draining the deoxygenated blood. The pampiniform plexus plays a significant role in thermoregulation of the testicles, as it helps to cool the arterial blood before it reaches the testes. Any disruption in the normal flow and function of these blood vessels can have implications for the health of the reproductive organs.
Pathophysiology of Epididymitis
Infectious Causes: Bacterial infections are a common cause of epididymitis. Pathogens such as Escherichia coli, Chlamydia trachomatis, and Neisseria gonorrhoeae can ascend from the urethra or bladder through the vas deferens to reach the epididymis. The presence of these infectious agents triggers an inflammatory response. The body’s immune system sends white blood cells to the area, which can lead to swelling, pain, and redness.
Non-Infectious Causes: Trauma to the scrotum, urinary reflux, or autoimmune disorders can also result in epididymitis. In cases of trauma, physical damage to the epididymis can initiate an inflammatory cascade. Urinary reflux can cause the backflow of urine into the epididymis, irritating the tissue and leading to inflammation. Autoimmune conditions occur when the body’s immune system mistakenly attacks the epididymal tissue.
Pathophysiology of Varicocele
Valvular Dysfunction: The most common cause of varicocele is the malfunction of the valves within the testicular veins. These valves are supposed to prevent the backflow of blood. When they fail, blood can pool in the veins, causing them to dilate and form a varicocele. This is often seen in the left testicular vein more frequently than the right due to anatomical differences.
Increased Intra-Abdominal Pressure: Conditions that raise intra-abdominal pressure, such as heavy lifting, chronic constipation, or even standing for long periods, can impede the normal venous return from the testicles. The increased pressure can force blood to back up in the testicular veins, contributing to the development of varicocele.
The Link between Epididymitis and Varicocele
Inflammatory Response and Vascular Changes: During epididymitis, the inflammatory process can affect the surrounding blood vessels. The swelling and increased pressure in the epididymal area may compress or disrupt the normal flow of blood in the adjacent testicular veins. This could potentially lead to changes in the venous pressure and valve function. For example, the inflammation-induced edema might create a local environment that increases the resistance to venous outflow, gradually straining the valves and predisposing to varicocele formation.
Immune-Mediated Mechanisms: In cases where epididymitis is due to an autoimmune disorder, the immune system’s abnormal activity might not be limited to the epididymis. There is a possibility that the immune-mediated attack could also target the endothelial cells lining the testicular veins. Damage to these cells can affect the integrity of the vein walls and the function of the valves, increasing the risk of varicocele.
Diagnosis and Evaluation
Clinical Examination: A physical examination of the scrotum is essential. In cases of epididymitis, the epididymis will typically be tender, swollen, and possibly have a hardened texture. For varicocele, the scrotum may feel like a “bag of worms” due to the enlarged veins. The doctor will also assess the size, location, and degree of swelling.
Imaging Studies: Ultrasound is the most commonly used imaging modality. It can clearly visualize the epididymis to detect signs of inflammation such as increased blood flow and swelling. For varicocele, it can show the dilated veins and assess the severity. Doppler ultrasound is particularly useful as it can evaluate the blood flow velocity and direction, helping to determine the functionality of the venous valves.
Treatment and Management
Treatment of Epididymitis: If the cause is infectious, antibiotics are prescribed based on the identified pathogen. For example, if it is a sexually transmitted infection, appropriate antibiotics like azithromycin for Chlamydia or ceftriaxone for Gonorrhea are used. In cases of non-infectious epididymitis, treatment focuses on addressing the underlying cause, such as providing pain relief and anti-inflammatory medications for trauma-induced cases.
Treatment of Varicocele: Mild varicoceles may not require immediate treatment and can be managed with lifestyle modifications such as wearing supportive underwear and avoiding activities that increase intra-abdominal pressure. However, if the varicocele is causing pain, infertility, or testicular atrophy, surgical intervention may be necessary. Surgical options include varicocelectomy, which involves ligating the affected veins.
Conclusion
In summary, while epididymitis and varicocele are distinct conditions, there is a potential link between them. The inflammatory and immune-mediated processes associated with epididymitis can have an impact on the testicular vasculature and potentially lead to the development of varicocele. However, this relationship is complex and not fully understood. Early diagnosis and appropriate treatment of epididymitis are crucial not only for resolving the acute symptoms but also for potentially preventing the long-term complication of varicocele. Healthcare providers should be vigilant in evaluating patients with epididymitis for any signs of developing varicocele and vice versa. Through continued research and clinical experience, a more comprehensive understanding of this relationship will emerge, enabling better preventive and treatment strategies in male reproductive health.
Related topics























